Cancer treatments: we must serve patients, not private interests
Published 4th February 2019
Dr Françoise Sivignon, President of Doctors of the World, France.
The number of new cases of cancer continues to rise, reaching 3.7 million a year in Europe. Behind this increase lies another equally worrying trend: the rising costs of new treatments. It is no longer unusual to see cancer treatments costing between €50,000 and €90,000 per patient, per year. Worse still, prices reached new heights a few months ago, with the introduction of CAR-T therapies, billed at between €300,000 and €350,000 per patient.
Given this situation, healthcare systems are finding it increasingly difficult to ensure everyone has access to the best possible drugs. The exorbitant sums charged for cancer drugs approved by States today will constitute barriers to accessing healthcare tomorrow.
In other words, at these price levels, healthcare systems will no longer be able to pay for every patient, forcing some to be excluded from treatment.
Abuse of the patent system
These exorbitant prices are made possible by a patent system that ensures industrial pharmaceutical companies can retain their twenty-year-old monopolies. Thus, it guarantees that there will be no competition from generic and biosimilar drugs. For sixty years, drug patents in Europe have been organised as a means of promoting research and development. This system has deviated significantly from its original principle and is now subject to abuse.
The fact is that the major pharmaceutical firms invest little in research. New compounds are actually created by start-ups, which are subsequently bought up at high prices – often in the region of billions of euros – by industrial drug companies. For example, Yescarta®, Gilead’s CAR-T therapy, was not developed by this firm but by a different company, Kite Pharma, which was acquired for 12 billion dollars in 2017.
Sixty years after their creation, pharmaceutical patents are now principally financial assets and a source of income and profits. Cancer research has become as much a potential growth sector as a battle for health. It is clear that the sums billed to States include the cost of any financial transactions relating to mergers and acquisitions.
When individual citizens pay their taxes and national insurance contributions, they are therefore also helping finance these speculative financial deals. By accepting drug costs based on the misuse of patents, States make themselves complicit in the abuse of public taxes for private gain, at the expense of the health and lives of those who are ill.
Putting access to care back at the heart of the system
None of this is inevitable, however. When arrangements for pharmaceutical patents were first put in place, States voluntarily adopted measures in the form of compulsory licensing to circumvent monopolies when public health demanded it. This tool, which has since been recognised in international law, is the reminder that a reciprocal condition of drug patents is the fundamental right to access health services.
It is the duty of governments to ensure that their healthcare systems are sustainable. To mark this year’s World Cancer Day, we are therefore calling on them to guarantee that access to healthcare for all takes precedence over the private interests of the few and to use the legal tools and means at their disposal to make this happen.





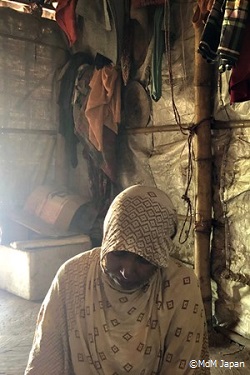 I am a TBA. When I was in Myanmar I was working at Malteser (German NGO). In addition to my role as a TBA, I was in charge of vaccination, polio treatment, and the like. Malteser’s clinic was the only free clinic we had. Other hospitals would only take patients who could pay an extra treatment fee. Poor people with severe illnesses and no money could only wait for death, without any medical treatment.
I am a TBA. When I was in Myanmar I was working at Malteser (German NGO). In addition to my role as a TBA, I was in charge of vaccination, polio treatment, and the like. Malteser’s clinic was the only free clinic we had. Other hospitals would only take patients who could pay an extra treatment fee. Poor people with severe illnesses and no money could only wait for death, without any medical treatment.
 First of all, I would like to thank Bangladeshi people and their government for their hospitality. They allowed us to live here. However conditions are very rough. If I could return to my original life, I would like to return to Myanmar immediately. Here, we get rice, beans and oil distribution and I think it is undoubtedly appreciated. But what about fish and meat? I cannot buy it because I have no job nor money. In the past, a clinic was nearby, but it disappeared without notice. It is quite troublesome not to be able to receive any medical care, but it is not our only issue. There are also no school. Children cannot receive education either. I want to return to Myanmar, we should be given legitimate citizenship, like the people of Bangladesh. I would like to be able to live in Myanmar with a legitimate status.
First of all, I would like to thank Bangladeshi people and their government for their hospitality. They allowed us to live here. However conditions are very rough. If I could return to my original life, I would like to return to Myanmar immediately. Here, we get rice, beans and oil distribution and I think it is undoubtedly appreciated. But what about fish and meat? I cannot buy it because I have no job nor money. In the past, a clinic was nearby, but it disappeared without notice. It is quite troublesome not to be able to receive any medical care, but it is not our only issue. There are also no school. Children cannot receive education either. I want to return to Myanmar, we should be given legitimate citizenship, like the people of Bangladesh. I would like to be able to live in Myanmar with a legitimate status.




